
Temperature management : bladder temperature (PCCU)
exp date isn't null, but text field is
Objectives
Temperature measurement is a commonly used assessment parameter when caring for acutely and critically ill children. In the critically ill child an abnormal temperature may reflect changes in their physiological status. Therefore, temperature measurement and temperature trends must be accurate and consistent, as decisions about therapeutic intervention may be based upon it. Pulmonary artery temperature measurement is still considered to be the ‘gold standard’ for measuring core body temperature. However, in practice this is too invasive and not a practical method of thermometry. Instead, body temperature is usually measured from a site, or ‘shell’ sites that are thought to reflect the core temperature. The site and measuring device chosen is based upon a number of factors including age, clinical condition, degree of accuracy required, safety and ease of use. It is responsibility of the nurse to determine the best method for monitoring patient temperature and to use the temperature monitoring device correctly. Whichever site/equipment chosen, the nurse must be aware of the benefits and limitations of each.
This nursing procedural guideline is intended as a resource for nursing staff involved in caring for children in the Paediatric Critical Care Unit at the Royal Hospital for Children, Glasgow that require monitoring and measurement of body temperature. The guideline has been constructed after literature search and review of sourced textbooks, Medline and CINAHL, and external nurse expert peer review and opinion.
Scope
This nursing procedural guideline is intended to be followed by nurses involved in caring for the highly dependent or critically ill infant or child requiring body temperature monitoring within the Paediatric Critical Care Unit at the Royal Hospital for Children, Glasgow.
Audience
All nursing staff involved in the measuring and monitoring of temperature in the Paediatric Critical Care Unit should be familiar with this nursing procedural guideline.
- Non-sterile gloves
- Disposable apron
- Suitable monitoring module and probe (E.g. Phillips monitor) (Fig1)

Fig 1. Phillips monitor
Equipment for catheterisation if appropriate urinary catheter with thermistor not already in situ (aseptic technique following ANTT):
- Sterile dressing pack
- Sterile gloves
- Sterile foil bowl
- Disposable apron
- 0.9% Sodium chloride – for cleansing
- Sterile lubricant gel – with local anaesthetic (E.g. Instagel®)
- Adhesive tape for fixing catheter or Clinfix®
- 5ml syringe & sterile water – for catheter balloon
|
PROCEDURE: |
RATIONALE |
|
Before any patient ‘handling’ or checking of monitoring probes, wash hands thoroughly with appropriate antibacterial skin cleanser and don apron and non-sterile gloves. Utilising an ANTT approach, prepare the child and equipment in order to protect all key parts and sites. |
To minimise the risk of cross infection. |
|
If the infant or child has been admitted to Paediatric Critical care with an appropriate adapted indwelling urinary catheter then connect the temperature probe into the specific monitoring module Provide age appropriate explanation to child (where applicable) and/or parents. |
To get an initial and baseline temperature recording.
To ensure the child (and parent) understand need for and consent to continued indwelling bladder probe use. |
|
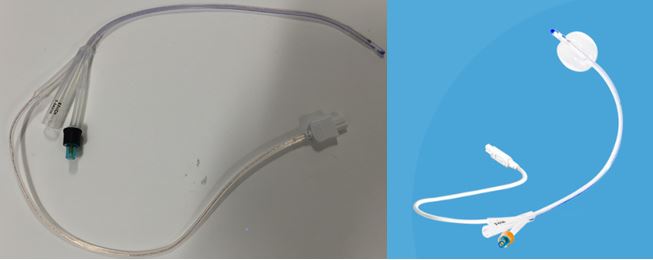
If no urinary catheter in situ and bladder temperature monitoring is required, then select appropriate catheter (see equipment & Fig. 2) and insert. (see separate guidance for urinary catheterisation).
|
Using an evidence-based guideline for urinary catheter insertion & care of urinary catheter should minimise the risk of associated complications such as urethral trauma, pain and cross infection. Using the urinary catheter insertion guideline will also help ensure the catheter (and temperature sensor) is in the best position to obtain a more accurate bladder temperature. |
|
When choosing a bladder temperature monitoring catheter, check disposable temperature measurement probe packaging is sealed and does not appear ‘used’ or opened.
Fig. 3 N.B Check expiry date on probe packaging prior to use. |
To ensure that the probe is sterile, unused, not broken, suitable for use and to minimise the risk of cross infection.
Temperature probe may no longer be sterile if out of date. |
|
Once the bladder temperature monitoring catheter is in the correct position it should be secured to the infant or child’s leg with non-irritant tape or device such as Clinifix®. (Fig 4) |
Securing the probe will help ensure it does not slip further in or out of the bladder thus affecting the temperature measurement and trend.
|
|
Connect the catheter temperature probe (Fig. 5) to the monitoring probe (Fig. 1)
|
Temperature will not be displayed unless bladder catheter temperature is connected to correct monitoring probe. |
|
The bladder temperature will be displayed continuously via the infant or child’s monitor and will automatically be recorded on the hour. Each hour the nurse should check and validate (if accurate) the infant or child’s temperature and the site - bladder. |
The Paediatric Critical Care unit Clinical Information System will record whatever temperature is being monitored. It will not take account of other factors that may lead to an inaccurate recording. E.g. if the catheter has slipped out or bladder lavage has been given. It is vital that the nurse checks the temperature ‘recorded’ and where from and adds additional comments or events where applicable. |






In certain circumstances, the bladder site for temperature measurement has been considered to be an accurate reflection and estimation of core body temperature in infants and children where it has not been possible to use a pulmonary artery catheter.
Bladder thermometry requires the use of a specific sterile, disposable indwelling urinary catheter with a temperature sensor running through the catheter. The temperature sensor is usually located 13mm from the catheter tip. Many infants and children in the paediatric critical care unit routinely have a urinary catheter in situ so the use of a catheter with a thermistor probe is no more invasive than a ‘normal’ catheter and if cared for correctly should cause no additional discomfort to the infant or child.
Bladder thermometry is used in paediatric, neonatal and adult intensive care units as well as during some operative procedures, as it is thought to provide a continuous temperature reading or trend without being influenced greatly by changes in ambient temperature. Some earlier studies have suggested that accuracy of bladder temperature monitoring may be influenced by urine flow rate. Whereas, other studies have found that bladder temperature remains reliable with changes in urine flow rate.
The nurse must be aware of the limitations of bladder thermometry if choosing this method of temperature monitoring. For example, urinary catheters with thermistor probes are available in a variety of sizes. However, the smallest catheter available at present is a size 8FG and may be too large for neonates and smaller infants less than 4kg.
Bladder thermometry readings may be unreliable and inaccurate where there are extremes of temperature and thermal flux such as during the cooling and warming phases of cardiopulmonary bypass. In shock states where there is poor perfusion to the lower abdomen and kidneys, or in the presence of fever, a ‘lag’ in bladder temperature reading, compared to other temperature sites (including pulmonary artery) has been reported.
There are documented risks when using bladder thermometry although these are related to the fact that the infant or child has an indwelling catheter. These include urethral trauma (from insertion), urinary tract infection, blockage and haematuria.
If the nurse finds any abnormal temperature measurements using bladder thermometry technique, then first check the catheter is still in situ. If the temperature reading appears accurate then this should be reported and documented. Another method & site of thermometry should also be considered.
Bray, L Sanders, C (2006) Nursing management of paediatric urethral catheterisation. Nursing Standard, Vol.20 (24), pp. 51-60.
Fallis, WM (2002) Monitoring urinary bladder temperature in the intensive care unit: State of the science. American Journal of Critical Care, Vol. 11 (1), pp 38-45.
Fallis, WM (2005) The effect of urine flow rate on urinary bladder temperature in critically ill adults. Heart and Lung, Vol. 34 (3), pp 209-216.
Fisk, J Arcona, S (2001) Comparing tympanic membrane and pulmonary artery catheter temperatures. Dimensions of Critical Care Nursing, Vol. 20, pp. 24-34.
Greenes, DS Fleisher, GR (2004) When body temperature changes, does rectal temperature lag? The Journal of Pediatrics, Vol. 144 (6), pp 824-826
Harris, C (2004) Best practice statement – Urinary Catheterisation and Catheter Care. NHS Quality Improvement Scotland, Edinburgh.
Kimberger, O Cohen, D Illivich, U Lenhardt, R (2007) Temporal artery versus bladder thermometry during perioperative and intensive care unit monitoring. Anesthesia and Analgesia, Vol. 105 (4), pp. 1042-1047.
Lamb, C & iMD-Soft (2009) C.I.S. Basic Help File, Yorkhill NHS Division PICU and HDU Clinical Information System (CIS), pp 12-13. NHS GGC, Glasgow.
Langham, GE Maheshwari, A Contrera, K You, J Mascha, E (2009) Noninvasive temperature monitoring in postanaesthesia care units. Anesthesiology, Vol. 111 (1), pp. 90-96.
Lefrant, JY Muller, L Emmanuel Coussaye, J Benbabaali, M Lebris, C Zeitoun, N Mari, C Saissi, G Ripart, J Eledjam, JJ (2003) Temperature measurement in intensive care patients: comparison of urinary bladder, oesophageal, rectal, axillary and inguinal methods versus pulmonary artery core method. Intensive Care Medicine, Vol. 29, pp 414-418.
Martin, S Kline, A (2004) Can there be a standard for temperature measurement in the pediatric intensive care unit? Advanced Practice in Acute Critical Care: Clinical Issues, Vol. 15 (2), pp 254-266.
Maxton, FJC Justin, L Gillies, D (2004) Estimating core temperature in infants and children after cardiac surgery: a comparison of six methods. Journal of Advanced Nursing, Vol. 45 (2), pp 214-222.
Moran, JL Peter, JV Solomon, PJ Grealy, B Smith, T Ashforth, W Wake, M Peake, SL Peisach, AR (2007) Tympanic temperature measurements: Are they reliable in the critically ill? A clinical study of measures of agreement. Critical Care Medicine, Vol. 35 (1), pp 1-10.
NHS Greater Glasgow Prevention and Control of Infection Manual: Urinary catheter care hub (2017) and Standard Operating Procedures: Insertion and maintenance of urinary catheters.
Nimah, MM Bshesh, K Callahan, JD Jacobs, BR (2006) Infrared tympanic thermometry in comparision with other temperature measurement techniques in febrile children. Pediatric Critical Care Medicine, Vol. 7 (1), pp 48-55.
Preston, RM (2005) Aseptic technique: evidence-based approach to patient safety. British Journal of Nursing, Vol. 14 (10), pp 540-546.
Robinson, JL Seal, RF Spady, DW Joffres, MR (1998) Comparison of esophageal, rectal, axillary, bladder, tympanic and pulmonary artery temperatures in children. The Journal of Pediatrics, Vol. 133 (4), pp 553-556.
Scottish Patient Safety Programme: Paediatrics (2015) SPSP Paediatric Programme Driver Diagram & Change Package.
Sessler DI (2008) Temperature monitoring and perioperative thermoregulation. Anesthesiology, Vol. 109 (2), pp 318-338.
Last reviewed: 09 May 2022
Next review: 09 May 2025
Author(s): Jeanette Grady
Version: 5
Approved By: PICU Guideline Group
Reviewer Name(s): L. Moore, M. McGale