
Acute Sore Throat
exp date isn't null, but text field is
Objectives
Guidance for the assessment and management of throat infections in children.
Scope
Children presenting to hospital (RHC) with a sore throat.
Audience
Medical and nursing staff assessing children presenting with sore throat in the ED and CDU at RHC.
November 2023: This guidance is currently under review as it has gone beyond the standard review date. It reflects best practice at the time of authorship / last review and remains safe for use. If there are any concerns regarding the content then please consult with senior clinical staff to confirm.
An acute sore throat is a common presentation to the paediatric emergency department. The majority of sore throats resolve within 1 week irrespective of the cause (40% within 3 days and 85% within 1 week)1. There are many causes of sore throats and it is important to identify the life-threatening causes as well as sore throat caused by Group A Streptococcus (GAS) as this needs antibiotics to prevent possible complications.
Sore throat can be bacterial, viral or non infectious (GORD, hayfever, smoke). The most common viral cause is rhinovirus (20%)3 and the most common bacterial cause is group A streptococcus (GAS)(10-30%)2
Clinical features alone do not reliably discriminate between bacterial and viral causes but can give us some guidance on diagnosis.
|
Symptoms suggestive of viral or GAS |
||
|
Viral |
Group A streptococcal (aged 1-3 years) |
Group A streptococcal (most common aged 3-14 years) |
|
Conjunctivitis |
Mucopurulent rhinitis |
Sudden onset sore throat |
|
Rhinorrhoea |
Excoriated nares |
Dysphagia |
|
Cough |
Diffuse adenopathy |
Fever |
|
Oral ulcers |
Exudative pharyngitis (rare) |
Headache |
|
Hoarseness |
|
Nausea and vomiting |
|
Rash |
|
Abdominal pain |
|
Diarrhoea |
|
Red swollen tonsils and uvula |
|
Wheeze |
|
Patchy exudates on pharynx |
|
|
|
Palatine petechiae |
|
|
|
Anterior cervical adenitis |
|
|
|
Scarlatiniform rash |
McIsaac score (modified centor criteria)2
The Centor criteria are only validated for adult patients in primary care and are not validated for children under the age of 3 due to the different clinical presentation of GAS in the first years of life. The McIsaac score (modified centor criteria) can be used in patients over 3 years old and takes into account the higher rate of streptococci in the 3-14 year age group. NICE recommends prescribing antibiotics if the patient scores 3 or more.
| History of fever | add 1 point |
| Tonsillar exudate | add 1 point |
| Tender enlarged cervical lymph nodes | add 1 point |
| Absence of cough | add 1 point |
| Ages 3-14 | add 1 point |
| Ages 15-44 | add 0 points |
|
McIsaac score |
Percentage risk of GAS4 |
|
0 |
1-2.5% |
|
1 |
5-10% |
|
2 |
11-17% |
|
3 |
28-35% |
|
4-5 |
51-53% |
The FeverPAIN criteria5,6,7
|
The Fever PAIN score was derived from a cohort study including 1760 adults and children aged 3 and over. The score was tested in a trial comparing three prescribing strategies, empirical delayed prescribing, use of the score to direct prescribing or combination of the score with use of a near patient test (NPT) for streptococcus. Using the score resulted in more rapid symptom resolution and reduced prescribing of antibiotics (both reduced by one third). The addition of the NPT did not confer any additional benefit. The score consist of five items:
Each of the FeverPAIN criteria score 1 point (maximum score of 5)
|
Please note most GAS infections self resolve without complications
|
Supparative Occur shortly after initial infection |
Non supparative Occur after few weeks-rare in UK |
|
Acute otitis media (most common) |
Acute rheumatic fever |
|
Quinsy (peritonsillar abscess) |
Poststreptococcal glomerulonephritis |
|
Retropharyngeal abscess |
Reactive arthritis |
|
Cervical adenitis |
|
|
Mastoiditis |
|
|
Acute bacterial sinusitis |
|
|
Septicaemia |
|
|
Meningitis |
|
|
Empyema |
|
Throat swabs
NICE recommends that throat swabs are not routinely taken. This is due to turnaround time of 48 hours, poor sensitivity and they cannot differentiate between infection and carriage.
A positive throat culture makes GAS more likely but a negative throat culture does not rule out diagnoses.
Children have a high rate of asymptomatic carriage of GAS (40%)8. Carriers have low infectivity and are not at risk of developing complications.
However our departmental policy is that if the child is being treated with an antibiotic for likely GAS then it is useful to swab their throats before treatment in case of failure to respond to antibiotics.
If EBV is being considered then viral throat swabs should also be taken.
Bloods
Bloods are not recommended to differentiate between bacterial and viral infections. However, if suspected EBV, then bloods can be taken as per EBV guideline.
Rapid antigen testing - Not currently routinely available in RHC ED.
A systematic review of RCTs9 reviewing rapid antigen detection test (RADT) for group A streptococcus in children with pharyngitis found that RADTs have high sensitivity and specificity for identifying GABHS infection. In studies that compared rapid antigen testing and throat culture, rapid antigen testing had a summary sensitivity of 85.6% and a summary specificity of 95.4% (based on very low-quality graded evidence).
Clinical bottom line - using RADT you can expect that amongst 100 children with strep throat, 86 would be correctly detected with the rapid test while 14 would be missed and not receive antibiotic treatment. Of 100 children with non-streptococcal sore throat, 95 would be correctly classified as such with the rapid test while 5 would be misdiagnosed as having strep throat and receive unnecessary antibiotics.
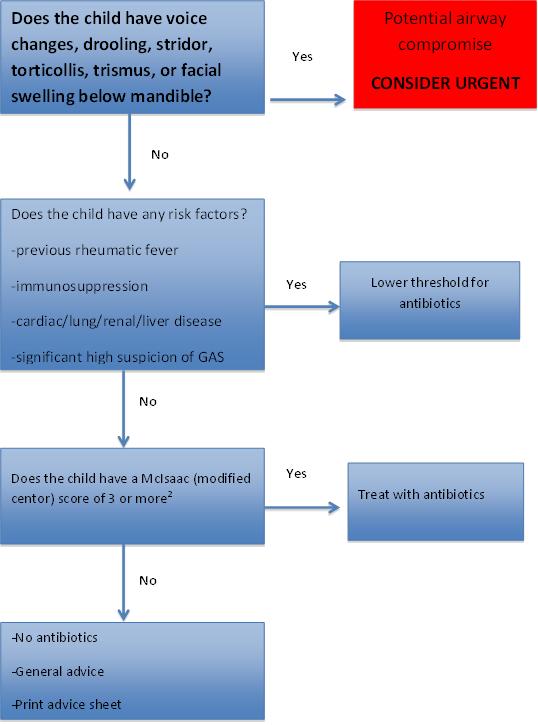
If the child has stridor, respiratory distress, drooling or is systemically very unwell they should be have urgent PICU review.
If the child is going to be discharged home then they should be given advice as below:
- Avoid hot drinks
- Take adequate fluid to avoid dehydration
- Gargle with warm salty water at frequent intervals until the discomfort and swelling subside (age appropriate)
- Suck throat lozenges, hard boiled sweets, ice or ice lollies
- Use Benzydamine spray (Difflam) (there is no good clinical evidence of effectiveness but many children find this helpful)
- Use Paracetamol first line with Ibuprofen as alternative
- Advise that if the child worsens or has a prolonged illness then they should be reviewed.
Antibiotics should be considered if a child over 3 years old has 3 or more McIsaac criteria and symptoms significant enough to warrant treatment. Phenoxymethylpenicillin or Clarithromycin (if true penicillin allergy) should be used. Antibiotics should be prescribed as per current NHS GGC empirical antibiotic guidelines.
There is no validated scoring system for bacterial tonsillitis in children under 3 years of age. Decision to treat this age group with antibiotics is based on clinical judgement.
Amoxicillin or Co-amoxiclav should not be used as this can cause a significant rash in patients with infectious mononucleosis.
|
Cause |
Symptoms |
Investigations |
Treatment |
|
Peritonsillar abscess (Quinsy) |
-severe sore throat often unilateral -hot potato voice -drooling -trismus -neck swelling -referred ear pain |
|
Discuss with ENT regarding IV antibiotics and drainage |
|
Epiglottitis or bacterial tracheitis
(more likely if not immunised against HIB)
|
-abrupt onset respiratory distress -absent cough with low pitched stridor -muffled/hoarse voice -tripod/sniffing positioning -drooling -fever |
-do not examine throat, do venepuncture or lateral neck x-ray in patients with severe respiratory distress due to risk of precipitating respiratory arrest
|
-early PICU review -maintain position of comfort with parents present -discuss with ENT regarding IV antibiotics |
|
Retropharyngeal abscess/lateral pharyngeal abscess |
Retropharyngeal -respiratory distress -stridor -dysphagia -odynophagia -drooling -torticollis -muffled voice -neck mass -trismus -chest pain Lateral pharyngeal -as above with swelling below mandible |
-lateral neck x-ray (normal does not exclude diagnosis) -CT with IV contrast with access to advanced airway management
|
-Early ENT +/- PICU review -Discuss with ENT regarding IV antibiotics
|
|
Infectious mononucleosis (glandular fever/EBV) |
-suspect if sore throat fails to improve/worsens -enlarged tonsils with thick white exudate -palatal petechiae -fever -generalised lymphadenopathy -fatigue/malaise -variable hepatosplenomegaly -amoxicillin induced rash -symptoms usually resolve in 1-2 weeks but lethargy can last months to years Complications -meningitis/encephalitis -hepatitis -myocarditis -orchitis -cytopenias -lymphoproliferation -splenic rupture |
-FBC, U+E, LFTs -glandular fever screening test (monospot)-may be negative in early phase and is unreliable under 4 years -EBV IgG and IgM - viral throat swab-(PCR for EBV specifically requested) |
-analgesia -hydration -consider corticosteroids
-if well and bloods normal-GP follow up with referral if still feverish in 1 week -if well and bloods mildly deranged-hospital follow up -if unwell then admit under medics and discuss with infectious diseases |
[10]
- NICE CKS-sore throat acute (Spinks, A., Glasziou, P.P and Del Mar, C.B (revised Jan 2018) Antibiotics for sore throat (Cochrane Review). The Cochrane Library. Issue 4. John Wiley &Sons, Ltd, thecochranelibrary.com
- Kanji K., et al, 2016. Antibiotics for tonsillitis: Should the emergency department emulate general practice?. Journal of clinical pathology. 69 (9), pp. 834-836
- Dynamed Plus. Pharangitis. http://www.dynamed.com/topics/dmp~AN~T114913/Pharangitis
- Escmid sore throat guideline group, et all, 2012. Guideline for the management of acute sore throat. Clinical Microbiology & Infection, 18 (Suppl 1), pp.1-28
- Little P, Stuart B, Hobbs FD, Butler CC, Hay AD, Delaney B, et al. Antibiotic prescription strategies for acute sore throat: a prospective observational cohort study. Lancet Infect Dis. 2014.
- Little P, Hobbs FR, Moore M, Mant D, Williamson I, McNulty C, et al. PRImary care Streptococcal Management (PRISM) study: in vitro study, diagnostic cohorts and a pragmatic adaptive randomised controlled trial with nested qualitative study and cost-effectiveness study. Health Technol Assess. 2014;18(6):1-102.
- Little P, Moore M, Hobbs FD, Mant D, McNulty C, Williamson I, et al. PRImary care Streptococcal Management (PRISM) study: identifying clinical variables associated with Lancefield group A beta-haemolytic streptococci and Lancefield non-Group A streptococcal throat infections from two cohorts of patients presenting with an acute sore throat. BMJ Open. 2013;3(10):e003943
- SIGN 117: Management of sore throat and indications for tonsillectomy (Feery BJ, Forsell P, Gulasekharam M. Streptococcal sore throat in general practice-a controlled study. Med J Aust 1976; 1 (26):989-91
- Cochrane Database Syst Rev. 2016 Jul 4;7:CD010502. Rapid antigen detection test for group A streptococcus in children with pharyngitis. Cohen JF, Bertille N, Cohen R, Chalumeau M.
- Royal Hospital Children Australia –Sore thoat guideline
Last reviewed: 05 June 2018
Next review: 31 October 2024
Author(s): Dr Ciara Duthie, GP trainee, RHC ED. Dr Steve Foster, Consultant in Paediatric Emergency Medicine, RHC ED (correspondence author).
Version: 3